INTRODUCTION
It is generally recognized that the health problems of the population are increasing although there is a rapid development of biological and medical sciences. As experts researchers mention, many of these problems could be avoided or at least reduce their consequences if the lifestyle and habits of people, were different to the early age in relation to physical activity and exercise. Moreover, the value of physical education in the education of the young generation as a regular sports activity broader popular masses (mass sport) results in the rapid development of physical education science. In the 1940s, the pioneers of fitness (Cureton, Bruno, Balke, and Peterb Karpovich) conducted empirical studies to investigate the effects of physical activity. Especially they studied the improvement in physical fitness in relation to the cardiovascular endurance and body composition. These studies led in 1978 to the adoption of the report on the American College of Sports Medicine (ACSM), which was primarily authored by Michael Pollock, who was interested to investigate the amount and the type of exercise needed to improve physical fitness (ACSM, 1988).
The same information, although modified slightly at the revisions of this reference (American College of Sports Medicine 1990, ACSM 1995), continued to be the main standard for improving fitness. These studies concluded that participation in physical activities has a significant effect on cardiorespiratory system. In fact the groups that had less physical activity than that recommended by the ACSM, did not differ significantly from the groups that were sedentary. At the same time, other epidemiological studies, investigated the risk factors of various health problems, especially for diseases of the heart. There have been several studies (Blair et al. 1989, Paffenbarger et al. 1986) that compared populations of lower or higher activity. The results showed that there is less risk of heart disease among the active groups as compared to the non-active groups.
In addition, other studies have investigated the relationship between the level of physical fitness and heart diseases or other problems. Haskel (1984) was one of the first experts, who noticed the relationship between physical activity and health. The (ASCM, 2008) reported briefly on the findings of laboratory research, about what should be done to bring about changes in the physical fitness of a person. Previous observations confirmed the importance of minimum activity level in order to reduce the high risk of cardiovascular disease in sedentary groups. The greatest decrease in risk factors of heart disease comes from the minimum activity. The gradually increasing activity and the higher levels of activity and fitness, showing the obvious benefits of reducing heart disease challenge probabilities.
There are many indications of the importance of primary prevention of cardiovascular disease (CVD), which is known that start from childhood. Studies autopsy performed on children and young people, after the unlikely deaths (PDAY, Research Group 1990, Newman et al. 1986, Berenson et al. 1998, McGill, et al. 2001), documenting the significant positive correlation between the established risk factors and the presence of atherosclerotic lesions in the aorta and the coronary arteries of children and young people. Recent data onto the Finland study (Raitakari et al. 2003) reaffirm the relationship between risk factors of childhood and adolescence and atherosclerosis during the adult’s life. Further longitudinal studies show the relationship between risk factors and cardiovascular diseases from childhood to adulthood of the individuals (Lauer & Clarke 1989, Lauer et al. 1988, Janz et al. 2000).
Epidemiological studies, among which includes the “Third National Nutrition Examination Survey”, (NHANES III), provide important data onto the prevalence of risk factors for the development of CVD and relate this trend behavior on health issues (Winkleby et al. 1999, Troiano et al. 1995, Ogden et al. 2002, Cook et al. 2003, Levin et al. 2003). These data are useful for giving information about individuals and devise the strategy to be followed for the improvement on public health. Also support the need for greater and more effective approach to the population of issues related to the cardiovascular health of children and young people. The data onto the physical activity from the same survey (Grunbaum et al. 2012), show that the percentage of students who exercised daily decreased from 43.7% in 2001 to 24.6% in 2011. According the students reported, only about one-third of them reported that exercised for 15 minutes or more during physical education classes. Moreover, participation in sports for recreation and entertainment decreased substantially from the ages of 7-11 years. This type of change is more intense and distinct among girls. Also in 2001, the YRBS study concluded that the rate of participation in girls in exercises and the maximum intensity was 63% in 8 years age and 41% at 11 years age (Grunbaum et al. 2002). Similar data from the longitudinal study “National Heart, Lung, and Blood Institute” (NHLBI), show that there is a sharp decline in physical activity during adolescence, between boys and girls (Kimm et al. 2002).
Also at the age of 18 and 19 years, 56% of the girls reported no physical activity in relation to sports or leisure. Notable factors that can predict the decrease in physical activity are the low educational level of parents and the high body mass index (Kimm et al. 2002). Overall, the available evidence points to the need for the individual and the overall approach from the population to primary prevention of CVD, which start from childhood. The guidelines of the American Heart Association (AHA) to improve cardiovascular health (Pearson et al. 2013) describe a comprehensive list of objectives, targets and strategies that can be reached from the general population. The Fitnessgram test battery is a set of assessment of fitness for young people. This method of fitness assessment developed by The Cooper Institute (Cooper Institute for Aerobics Research, CIAR) and responds to the existence of the need for a comprehensive evaluation of physical education programs. The assessment includes a variety of health-related tests, which were designed to evaluate the cardiorespiratory endurance, muscular strength, muscular endurance, flexibility and body composition. Benchmarks have been established for children and young people for each of the categories related to the physical condition (CIAR 1999).
The Cooper Institute developed the Fitnessgram test in 1987 and was recognized and certified by the American Alliance for Health, Physical Education, Recreation, and Dance (AAHPERD). The primary purpose of the Fitnessgram battery test was to help students and establish physical activity as part of their daily lives. Tests of Fitnessgram package provide students with a number of options so it gives to everyone the opportunity to participate. This possibility of the existence of alternative tests that can examine and score the same parameter is particularly important at the assessment of physical fitness, because it gives more opportunities to complete all tests.Also, the package can be used by teachers to assess the needs of students and to help themselves to the design of physical education programs. Finally it can be used by parents to understand the needs of their children and to help in the planning of their physical activities (CIAR 1999).
Each test of Fitnessgram battery is chosen to calculate and assess some important aspect of health and not some skill. Students are not compared with each other, but with special standards, relating to health, which has been carefully verified for each age and sex. Participants receive objective, personal feedback and positive reinforcement, which is essential to change behavior and that essentially plays the role of the communication link between the teacher and the parents. Finally the Fitnessgram test battery emphasizes the participation in various physical activities for the development and maintenance of an acceptable fitness model. Four main fitness factors can be measured by the test Fitnessgram: the aerobic capacity, the body composition, the muscular strength and the endurance and flexibility.
Fitnessgram test battery uses specific benchmarks to assess the physical fitness. These standards have been established in such a way that the appropriate level of fitness can offer a degree of protection against disease and sedentary lifestyles. The performance of each individual is classified into two general areas, the “health zone” in the zone that “needs improvement”(CIAR 1999). As it was reported, a score belonging to the “health zone” represents a level of fitness that offers some protection from potential health risks. These standards reflect a reasonable level of fitness, which can be obtained from the majority of children that regularly participate in a variety of exercises, or involving themselves in physical activities. For this reason it is recommended to all students strive to achieve a score which will rank them among the health zone limits. It is not uncommon many students to achieve appropriate levels in some categories, while not succeed in others. In many children there are areas which are doing much better than others (CIAR 1999).
The category below the level of “health zone” referred as “needs improvement” and indicates that the physical condition of the person may need special attention. While the results of the low level of fitness may not affect health into adulthood, it is important to identify future risks promptly. Thus the level of fitness “needs improvement” can be used sliders to help children that they set new goals, to improve their level of fitness (CIAR 1999). The development of standards for physical fitness in young people (children and adolescents) is relatively recent. Until now the question about the amount of physical activity that is necessary to young’s is not answered satisfactorily. But surveys show the importance of being able activity for health (Bouchard et al. 1990, Department of Health and Human 1980, Haskel et al. 1985, Malina, 1990) and the belief that intervention at an early age is important to maintain the active lifestyle in later life (Haskel et al. 1985, Pate & Blair 1978, Simons et al. 1988).
The best indicator for cardiopulmonary endurance is considered the aerobic capacity. Acceptable aerobic capacity levels correlate with the decrease of elevated blood pressure and reduce the risk of coronary heart disease, obesity, diabetes, certain cancers and other health problems (Safrit et al. 2000). Aerobic capacity consider the ability of the heart, lungs and circulatory system to receive oxygen from the atmosphere and expelling the carbon dioxide produced in the cells of the body in energy process. Whereas the level of aerobic capacity and assessing the level of physical activity, support the maintenance of good health throughout the duration of the remaining life (Blair et al. 1989, Karvonen 1982, Paffenbarger et al. 1986), which must be accompanied by a growing interest in the fitness early in the school age (Pate 1989, Whitehead et al. 1990). For the measurement of aerobic capacity it is used the lab, where the maximum amount of oxygen that one needs when performing a maximum muscle effort (usually running on the treadmill or the ergometer). However, it is more practical, and equally accurate to assess the aerobic capacity in school or observing the total distance covered in 9 or 12 minutes run-walking or observing the total time needed for a running or walking 1 or 1.5 miles.
Muscular endurance and strength are important factors related to health and fitness. According Westcot (1991), four out of five Americans have felt discomfort in the lower part of back and 80% of these problems are muscular nature that can be corrected by power drills. Studies of Kibler et al. (1992) and Stone (1990) show that the strength exercises reduce the risk of injuries in the joints or muscles, which can occur during physical activity. Muscle strength is measured more accurately in the laboratory using a dynamometer the entasiometro or the Cybex machine. However, many muscle strength and muscle strength measurements may be held outdoors, such as school, with relative accuracy.
The most common measurement for the flexibility is the test by folding the seat position, used in fitness related to health. The fold test from the home location, based on the significance of the findings on the role of the flexibility of the body in preventing diseases of the lower part of the lower back (Jacson & Balker 1986, Kraus & Raab 1986). So this test has incorporated almost in every national fitness test including the American Alliance for Health Physical Education Recreation and Dance (AAHPERD), Physical Best (AAHPERD 1988), The President Council on Physical Fitness and Sport (PCPFS 1990), The Fitnessgram (Institute for Aerobics Research). The test normally used in schools, but there is a concern about whether a higher score indicates a greater flexibility or whether the relationship between the length of the hands and the length of the feet affect the score of the fold from the home location.
The body composition is considered as an indicator of the weight percent from fat. Maintaining proper the body composition is crucial for the prevention of obesity, which is associated with increased risk for diseases such as coronary heart disease. As a large percentage of body fat can be unhealthy also and the small percentage of fat may pose a health risk someone. Since the late 1970s, various interventions programs have been conducted, which aim to promote health in schools. Many of these interventions contained health literacy issues related to the heart, while in others intervened simultaneously in other risk factors for cardiovascular disease. Many of the early studies are considered to belong to the first generation, which were primarily teaching interventions and focused on the positive effect of the provision of knowledge on health issues or behavioral issues and attitudes. Since the mid 1980s the research was based on the school environment, focused and theoretical contributions from behaviors, but also evaluated and measured a number of factors were considered responsible for the occurrence of cardiovascular disease (Resnicow & Robinson 1997).
The results of this second generation of the surveys reviewed, analyzed and synthesized by Resnicow and Robinson, (1997), demonstrating the ability of these interventions in schools to improve risk factors for CVD in children and young people. Also documented investigations on the third generation, in which the investigation was extended beyond the classroom with interventions that focused on the wider school environment and included the nutrition and physical activity programs, which could be extended to other hours of the expiry school hours. Example of the third generation of the speeches is the CATCH research conducted in schools (Luepker et al. 1996, Dwyer et al. 1996, Edmundson et al. 1996, Lytle et al. 1996, Nader et al. 1999). A result of the CATCH intervention was a significant increase in the proportion of medium physical activity intensity during the school physical activity from 37% to 52% of students, with students in the intervention schools to be more physical activity to schools control (Luepker et al. 1996).
According to the research there are many intervention programs implemented in order to improve physical fitness. In Robinson’s research (1999) took part children aged 9-11 years. Children belonging to the intervention group were taught during the six months that lasted the intervention eighteen 18 theoretical courses, which were designed to reduce TV viewing, video and games. The total number of participants in the intervention group was 106 people. The control group, which consisted of 121 people, attended the typical school subjects. After the end of the program students were followed for a period of seven months. The results showed a significant reduction in BMI in the intervention group. Significantly greater reduction was observed in the intervention group in skin folds triceps muscle and waistline. In research of Muller et al. (2001) the intervention was done in schools by trained educators who tried to give the following message to the student, that they must have physical activity at least an hour a day and that should reduce watching TV in less than an hour day. At the end of the intervention it was found that there was a significant reduction in the BMI and skin fold thickness of the triceps muscle.
In research of Epstein et al. (1995) took part in obese people aged 8-12 years and their parents. There were three different groups. In the first group, emphasis was placed on reducing sedentary life, in the second group it was given emphasis on increasing physical activity and at the third group was given emphasis at the same time to increase physical activity and reduce sedentary lifestyles. The duration of the intervention was 4 months. The results showed a reduction in the intervention groups compared with the control group, the percentage of overweight and the percentage of body fat. In research of Epstein et al. (2000) that took part in obese people aged 8-12 years. In the control group participants were encouraged to reduce their sedentary lifestyle. Both groups followed the program for six months. The results showed that the pursuit of the objective of reducing sedentary behavior and increasing physical activity resulted in a reduction in the rate of obesity and body fat and improve aerobic capacity. Generally, the results suggested that reducing sedentary works positively towards reducing childhood obesity.
The purpose of the study was to evaluate the efficacy of a school based intervention program during the physical education lessons to improve the levels of physical fitness, using the Fitnessgram test battery (one-mile run/walk test, back saver sit and reach test (BSSR), trunk lift test, curl up test, and Body Mass Index) of students 12 and 13 years old.
MATERIALS AND METHODS
Participants
The sample consisted of 141 students (61 boys and 80 girls) aged 12 and 13 years old. (Table 1). They were from two schools of Central Greece region. The investigation excluded students who regularly practiced in sports teams or clubs or exercised regularly in private gyms or follow any form of training program.
Table 1: Number of students by age and sex
Table 2: Paired samples statistics for the fitnessgarm tests of the intervention between initial and final measurement
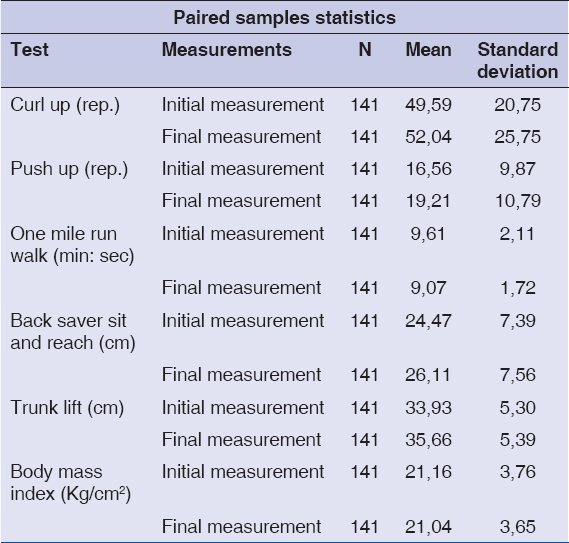
Table 3: Paired samples correlation for the fitnessgarm tests of the intervention between initial and final measurements
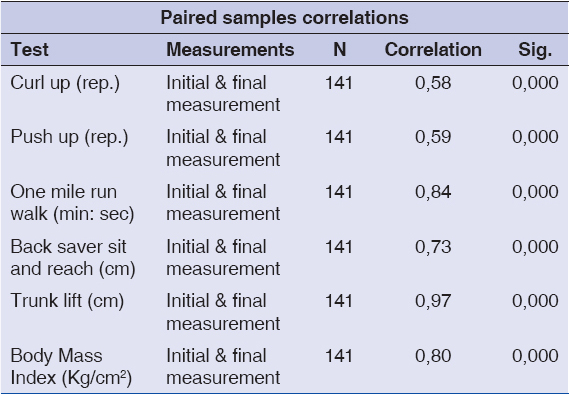
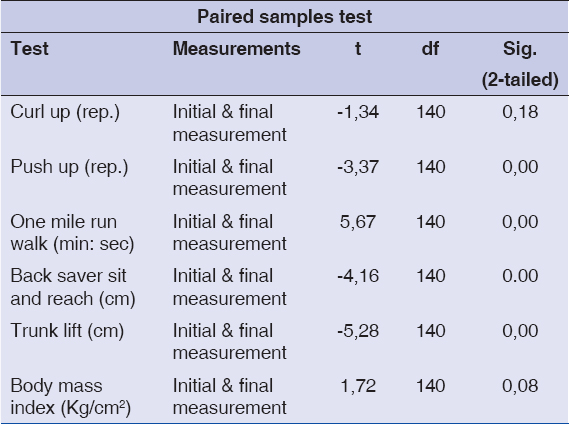
Table 4: Significant differences for paired sample T test for the fitnessgarm tests of the intervention between initial and final measurements
Implementation of the School Program
For the implementation of the course of physical education according to the timetable of the school program, responsible was the physical education teacher. The physical education teacher was responsible in both the experimental group schools and in the control group schools. Children who participated in the control group were not taught any particular object, but they followed a typical fitness program during physical education classes. The duration of the intervention program in schools was about 10 months. The frequency of the exercise program identified with the frequency of weekly hours of physical education in high school. More specifically, for students in the first grade and the second grade of high school, the exercise frequency was three times a week, while for students of high school, the frequency of exercise was 2 times a week. The duration of daily exercise training during the physical education lesson ranged from 35-45 minutes, depending on the timetable of the class program. Special attention was given from the physical education teacher at the intensity of aerobic exercises which should range from 40% to 60% of maximum heart rate during the physical education lesson.
Measurements
For the evaluation of the effectiveness of the intervention program, a series of tests were conducted at the beginning and at the end of the implementation of the program.
Measurement Procedure
Anthropometric measurements
Height and weight were measured with the students wearing light clothing and without shoes. Height was recorded to the nearest 0.5 cm and weight to the nearest 0,5 kg.
Body mass index (BMI) It was calculated as weight (kg) divided by height squared (m2) per age and sex specific cut off points (20). Cole et al. (2000).
Physical fitness
The Fitnessgram tests that used were the one-mile run/walk test, the 90 degree push up test, the back saver sit and reach test, the trunk lift test and the curl up test.
One-mile run/walk test
The test measures the cardio-respiratory endurance. The purpose is to walk or run a mile distance as fast as possible. 90o push up test. This test measures the upper body muscular strength and muscular endurance (muscle fitness). Push-ups are done in a slow rhythmical pattern, with arms lowered to ninety-degree angles, with the back and legs straight. Girls executed the push up test using their knees to support the body. The test objective is to complete as many push-ups as possible at a rhythmic pace.
Back saver sit and reach (BSSR) test
This test measures the joint flexibility, which is important for functional health. The objective purpose is to reach the specified distance on the right and left sides of the body.
Trunk lift test
This test measures low back muscular strength and flexibility. The objective of the test is to lift the upper body off the floor using the muscles of the back and hold this position for some seconds.
Curl up test
This test measures the abdominal strength and endurance. The objective of this test is to complete as many curl-ups as possible.
Statistical Analysis
Paired samples t tests were used to assess mean differences in the scores of the Fitnessgram tests (curl up test, push up test, one mile run walk test, back saver sit and reach test, trunk lift test and Body Mass Index), before the intervention and at the end of the intervention program. A level of 0.05 was used to determine statistical significance for each of the t tests and a Bonferroni correction procedure was applied. The data were analyzed using the Statistical Package for the Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA). A p-value of <0.05 was considered statistically significant.
RESULTS
A total of 80 females and 61 males (Table 1) were analyzed. A paired-samples t-test was conducted to compare the score of the curl up test before the intervention and at the end of the intervention program. There was not a significant difference before the intervention program (M=45,59, SD=20,75) and at the end of the intervention program (M=52,04, SD=25,75) conditions t(140)=-1,43, p=0,18. These results suggest that the intervention program really does have not had any effect at the score of the curl up test. For the push up test, a paired-samples t-test was conducted to compare the score of the push up test before the intervention and at the end of the intervention program. There was a significant difference before the intervention program (M=216,56, SD=9,87) and at the end of the intervention program (M=219,21, SD=10,79) conditions t(140)=-3,37, p=0,001. These results suggest that the intervention program really have effect at the score of the push up test.
For the one-mile run/walk test, a paired-samples t-test was conducted to compare the score of the one-mile run/walk test before the intervention and at the end of the intervention program. There was a significant difference before the intervention program (M=9,61, SD=2,11) and at the end of the intervention program (M=9,07, SD=1,72) conditions t(140)=5,67, p=0,000. These results suggest that the intervention program really does have an effect at the score of one-mile run/walk test.
For the back saver sit and reach, a paired-samples t-test was conducted to compare the score of the Back saver sit and reach test before the intervention and at the end of the intervention program. There was a significant difference before the intervention program (M=24,47, SD=7,39) and at the end of the intervention program (M=26,11, SD=7,56) conditions t(140)=-4,16, p=0,000. These results suggest that the intervention program really does have an effect at the score of Back saver sit and reach test.
A paired-samples t-test was conducted to compare the score of the trunk lift test before the intervention and at the end of the intervention program. There was a significant difference before the intervention program (M=33,93, SD=5,30) and at the end of the intervention program (M=35,66, SD=5,39) conditions; t(140)=-5,28, p=0,000. These results suggest that the intervention program really does have an effect at the score of trunk lift test.
Finally a paired-samples t-test was conducted to compare the score of the Body Mass Index before the intervention and at the end of the intervention program. There was not a significant difference before the intervention program (M=21,16, SD=3,76) and at the end of the intervention program (M=21,04, SD=3,65) conditions t(140)=1,79, p=0,086. These results suggest that the intervention program really does have not have any effect at the score of Body Mass Index (BMI).
CONCLUSION
The present study was designed to study the effect of an intervention program in schools to improve the parameters of the physical fitness (aerobic capacity, strength and flexibility). The current study has shown that the school is an appropriate setting in which students can improve their physical fitness, that is related with health, during the physical education lessons. At this study the intervention included a curriculum-based workshop for all pupils. Improving the level of physical fitness through the course of physical education in school and the correlation with health is important because it leads to increased interest of the students and motivate them to increase their physical activity.
Also, the proper design, the implementation of similar programs, the evaluation of the intervention program helps the teachers of physical education, to set objectives, a process necessary for the achievement of learning (Pemberton, 1995). Risk factors for cardiovascular diseases in childhood influence health in adulthood (Harsha, 1995), and emphasize the need for maintaining and improving physical education for health. Evaluation of intervention programs is only part of the education process in the course of physical education in schools, for improving the fitness of students that promotes health. An efficient intervention program at school level during the physical education lesson, should develop equally all elements of fitness related to health (Pangrazi et al. 1996)
According to our results the Body Mass Index was not significantly reduced at the students who participated in our study. The results are consistent with the meta-analysis of Harris and his associates (2009), which evaluated the effectiveness of educational interventions on Body Mass Index. Among 18 studies involving a total of 18.141 students the meta-analysis showed that BMI did not improved during the interventions. Our study results do not agree with the survey of Tamir and his collaborators (1990) that took place in Jerusalem, with duration of 2 years and used a modified version of the American program “Know your Body”. It was found to be a reduced of the Body Mass Index at students in the experimental group. The results showed that it is possible to reduce the Body Mass Index after an appropriate training of students in school.
On the results of the study to improve the flexibility of the students who participated, it proved that there really was better because the scores of tests that assess flexibility were better at the end of the program. The results agree with the results of the study of Stephens et al (1998) in which ninety-nine students received a 15-week intervention program for three times a week, obtained field measurements among other the sit and reach test for flexibility. At the end of the intervention program the supplemental activity group showed significant improvements in flexibility, body composition.
Regarding the aerobic capacity of students at the lesson of physical education which was assessed by the test of one mile run walk, it was improved that there was a significant improvement at the end of the intervention program. The present study agree with other surveys such as the investigation of Kriemler and his associates (2010), lasting one school year, in order to assess the effectiveness of a curriculum in 15 schools and 540 students that were selected randomly, and performed physical program activity included suitably modified physical education lessons (3 per week). It was measured risk factors for developing cardiovascular risk factors and among other factors the aerobic capacity and results showed increasing aerobic capacity and physical activity. Also the present study agree with the results of the intervention of Laparidis et al. (2010), with a sample of 343 students aged 12–16 years and duration of intervention for 1 school year. Among others parameters that were measured VO2max found to improve during the intervention lesson of physical education in school.
For the effective exercise of the elements of the physical fitness the time provided by the curriculum of physical education course is not enough. The Pangrazi and colleagues (1996) suggest that the development of fitness can be achieved through practice basic motor skills that are related to health. The physical education teacher can help in this direction guiding and controlling the continuation of the activity of children outside the school environment.
It is necessary for students to practice in order to improve their physical fitness related to health. For this reason, it should be given special attention and care to improve physical fitness through the proper education during school hours in the lesson of physical education. Clearly more research is needed, particularly in Greece to establish effective programs on improving fitness in adolescents. There is need for development and evaluation of such programs beyond school boundaries in the families and in society. But because it is crucial to maintenance of any changes in physical activity additional studies are needed to stabilize and maintain the positive results that may arise.