INTRODUCTION
Sports participants are at risk for unique and distinct kinds of dental injuries. Direct trauma from a highvelocity object, such as a baseball or (field) hockey ball that strikes the front teeth, is likely to cause a fracture. High-velocity trauma is more likely to fracture the teeth, whereas low-velocity trauma causes the greatest damage to the hard and soft tissues that surround the teeth. Any traumatic dental injury has the potential to challenge pulp vitality even if not apparent initially.
The resulting number of sports-related injuries was the occasion for numerous studies on the need to wear a mouthguard during several sporting activities. The first historic use of gum shields was found 1913 in the British boxing sport. This historic gum shield was made from natural rubber, which was held in position by keeping the teeth together. 1962 determined the “American Dental Association” the obligatory wearing of a mouthguard in US high school football. Guidelines for mouthguard use in sports have been developed by the Academy for Sports Dentistry and the American Academy of Pediatric Dentistry (1, 2). The National Collegiate Athletic Association requires the use of a mouthguard in 4 sports (football, ice hockey, field hockey and lacrosse), and the American Dental Association recommends the use of mouthguards in 29 sports and fitness activities (3). The German Society of Oral and Maxillofacial Surgery (DGZMK) recommends at least 15 sports, among others, handball, basketball and hockey, the wear of a mouthguard (4). Knapik (2007) performed studies on the physical properties and materials of a mouthguard (5). Earlier they were even of simple latex rubber, but today they are produced from different plastics such as polyurethane, ethylene-vinyl acetate (EVA) or polyvinyl chlorides. Often they are made from compounds of plastics, which give the mouthguard both elastic and rigid properties.
Generally 39 % of all oral and dental injuries are sportsrelated. Basically all sports with risk of falling, player contact and devices, especially balls or hockey sticks, have an increased risk for teeth and jaws. Even small forces can damage or fracture the teeth. A tooth can already brake when a compact plastic ball of 160 g (hockey) from a height of 2 meters simply bounces on the mouth without active acceleration. According to the Dental Association in Schleswig-Holstein, Germany, an efficient, comfortable, and properlyfitted mouthguard can reduce the sports-related dental injuries up to 60 %. It protects tongue, lips and cheeks against bite-lesions. The mouthguard absorbs blows and shocks due to its elasticity. On the other hand it is rigid enough to spread the energy away from the teeth to larger surfaces. In consequence of shock absorbency and force distribution alveolar and dental fractures are minimized, and concussions occur up to 16 fold fewer. An absolute indication for a mouthguard is an overjet greater than 3 mm or an insufficient lip-closing. A reduction in dental injuries has been demonstrated in sports where mouthguard use is mandatory, such as American football and ice hockey (6-8). In an in vitro animal model, the force required to damage dento-alveolar structures was increased by 14-fold for the permanent dentition (9) when a mouthguard was worn. The action of mouthguards in reducing extra-oral injuries has been demonstrated using lateral cephalometric radiographs. With a mouthguard in place, the mandibular condyles are positioned anteroinferiorly, preventing normal closure. This significantly reduces the risk of concussion following traumatic closure of the mandible, especially in individuals predisposed to such injury (10, 11). Although sportsrelated dental injuries cannot be eliminated entirely, many can be reduced in severity or prevented with the use of a properly fitted mouthguard (12-15).
Despite the clear potential of mouthguards to reduce the risk of injury, many athletes do not use them. They believe mouthguards inhibit breathing, gas exchange, and communication. There are different models of mouthguards available. We tested two commercially available models (one boil-and-bite vented and one custom fit two-component mouthguard) because they may be used more frequently than professionally fitted individual ones due to extreme differences in cost and accessibility.
It is the intention of the present study to check the wear, comfort and subjective impressions of mouthguards in athletes, who do not contact (volleyball), contact directly (field hockey) or indirectly (handball) with competition rivals. Players' knowledge, attitudes, and current mouthguard use need to be determined in order to direct educational resources and develop effective promotional messages.
There are 5 major aims of the present study: to check the use of mouthguards by these players and their reasons; to assess the comfort and wear characteristics of the two mentioned mouthguard types in handball and basketball in games and a sports specific agility test; to compare the regularly worn mouthguard of the field hockey players with the rating of the two mouthguards offered in our study; to assess a possible difference between the wear characteristics; and to describe the players' experience in orofacial injury.
METHODS
Experimental Approach
The experimental part of the present study in handball and basketball players used a within-subject repeatedmeasures design. The subjects had to report on two days twice (morning and afternoon). At first, subjects were informed about the experimental procedures and provided with both mouthguards used in this investigation. The experimental sessions occurred on two consecutive days. The subjects completed a series of physical agility tests and a match. During all activities, subjects wore the predetermined mouthguard assigned to that experimental session. In the basketball and handball groups the experimental sessions were applied in a randomized counterbalanced way. After each session a questionnaire was completed by the players to assess the comfort and possible complaints in the use of the two different types of mouthguards. No experimental session was conducted with the field hockey players. They completed a questionnaire about the comfort and possible complaints of their usually worn mouthguard.
Subjects
45 subjects were enrolled in this study by completing a consent form. Players recruited were male youths from the handball A-team of Sports Club Magdeburg (17-19 year olds, elite, n= 14), male adults from basketball (Second league, Leipzig (19-37 year olds, n= 8), and 19 female and 4 male youths and adults from Hockey Club Leipzig (all levels; social to elite: 9-12 year olds (n= 8), 15-19 year olds (n= 6), 20-30 year olds (n= 5), and over 30 (n= 4)).
Mouthguards
The purpose of this investigation was to describe the impact of boil-and-bite mouthguards on comfort and subjective impressions. Boil-and-bite mouthguards may be used more frequently than a custom-fitted model because of relevant differences in cost and accessibility. The mouthguards provided in the present study were the commercially avaiable vented boil-andbite mouthguard (VentMG), and the two-component custom fit mouthguard (MixMG), applied in the handball and basketball groups. All mouthguards were fitted to the participants by one dentist using the instructions provided on the packaging.
During the VentMG condition, the handball and basketball players wore a Nike adult max intake convertible mouthguard (Nike, Beaverton, OR, USA). This mouthguard has breathing channels designed to improve ventilation and gas exchange during sports performance. The mouthguard was placed in boiling water for 30 seconds, taken out and the water was gently shaken off. Then the mouthguard was carefully placed in the mouth to cover the upper teeth, and the subject was instructed to firmly bite down. Moderate pressure was placed on the lips and cheeks for 30 seconds. The mouthguard was then removed and washed with cold water.
During the MixMG condition, the custom fit twocomponent mouthguard (MixMG) was prepared according the packaging instructions. Powder and liquid were mixed with a spoon to a soft mass, then filled into a plastic occlusal template and placed in the mouth to cover the upper teeth. This mouthguard type was chosen because the soft mass adapted perfectly to the contour of each tooth, hardened in the mouth and got individualized. Excessive material and sharp contours were removed.
None of the described versions was used in the field hockey players since they used their regularly worn mouthguard (Dita Multi Sport Senior or Junior) and reported about the comfort and reasons of wearing.
Questionnaires
First a questionnaire was used to ascertain the mouthguard wear, awareness, attitudes and the reasons for using and not using in all 45 players (handball n= 14, basketball n= 8, field hockey n= 23). Additionally the dentofacial trauma experience was asked by the questionnaire. The incidence of trauma was recorded over the entire career of an athlete (usually retrospective). Similar questions have been used in previous study (16).
The second questionnaire assessed the comfort, subjective impressions, and complaints of mouthguard wear. The questionnaire was administered once to the field hockey players and twice to the handball and basketball players to evaluate both provided study mouthguards. In a scale from 0 (bad) to 10 (excellent) the mouthguard was categorized concerning fit, stability when running, comfort, interference in breathing, speaking, and drinking. In a scale of 0 (not at all) to 5 (extremely) the players should evaluate the mouthguard for possibly resulting dry mouth, thirst, burden, nausea, and retching.
Statistical Analysis
All data are presented as means ± SD. Analysis of groups was done using the Mann-Whitney U test, and independent t-test. A p-value of p < 0.05 was considered to indicate significance, and p < 0.005 as very significant. All analyzes were performed using the program Statistical Package of Social Science (SPSS) Version 21.0.
RESULTS
Mouthguard Wear Characteristics
In field hockey, 82.6 % (n= 19) used a mouthguard. Knowledge of the protective role of a mouthguard was the main reason for the use in field hockey (85.7 %), followed by the reason that other players had one (9.5 %), and advice by another player (4.8 %). The most frequent sources of mouthguard advice were club, trainer, and team members (66.6 %), followed by family and friends (29.2 %). The only female player, who had a professionally fitted mouthguard, had made up her decision for the use after an injury of a team member. A boil-and-bite mouthguard (Dita Multi Sport), provided by the hockey club, was used by 18 players (78.3 %). The age of the mouthguards differed between less than 6 months (42.1 %), 6-12 months (31.6 %), and 2 years and over (26.3 %). Mouthguard wear was less frequent in training (36.8 %; always) than at games (84.2 %; always). The most frequent reasons for not always wearing a mouthguard in field hockey were “speaking interference” (30.6 %), followed by “breathing interference” (22.2 %), “ uncomfortable to wear” (16.7 %), “never thought about it” (13.9 %), “not at high risk for dental injury” (8.3 %), and “friends don't wear them also” (5.6 %). Two female players reported that the wearing is a purely mental thing, because they feel uncomfortable in the game without a mouthguard. 19 (82.6 %) from 23 field hockey players believed in the protective role of mouthguards, 4 were unsure. 68.2 % found it necessary to wear a mouthguard in training sessions, 18.2 % not, and 13.6 % were unsure. In games found 81.8 % the wear of mouthguards necessary, 9.1 % not, and 9.1 % were unsure.
In basketball, only one from 8 basketball players reported to wear a professionally fitted mouthguard due to an earlier tooth fracture; none of 14 handball players had used a mouthguard before. The most frequent reasons of the basketball players to use no mouthguard were “never thought about it” (30.8 %), followed by “uncomfortable to wear” (23.1 %), “speaking interference” (15.4 %), and 7.6 % each “breathing interference”, “not at high risk for dental injury”, and “a lot of effort”. All basketball players believed in the protective role of mouthguards for orofacial injury, 4 thought that mouthguards are necessary in matches, and only one player thought mouthguard wear is necessary in training sessions, 3 were unsure for mouthguard use in training and one to use wear at games.
In handball, the most frequent reasons to wear no mouthguard were “never thought about it” (27.2 %), followed by 13.6 % each “breathing interference”, “speaking interference”, “not at high risk for dental injury”, and 13.6 % gave no answer. One handball player mentioned the uncomfortable wear and anotherone answered that “friends also don´t wear a mouthguard”. 10 (71.4 %) from 14 handball players believed in the protective role of mouthguards, 3 were unsure and one abstained. Only 2 players thought that mouthguard use might make sense in games, no one thought this for training. 7 players were unsure and one abstained.
Figure 1 shows the attitudes of players in handball and basketball toward mouthguard use in training and games. Nevertheless a majority of the total participants (81.8 %) advocates the general usefulness of mouthguards in protecting teeth and jaws.
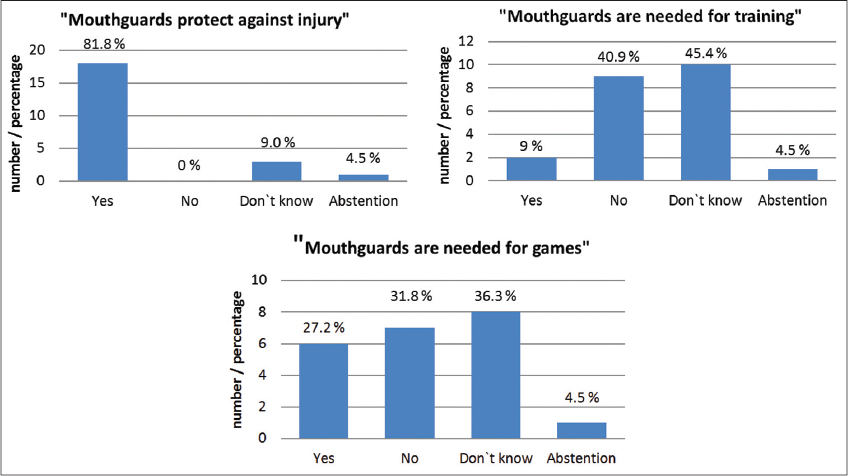
Figure 1: Attitudes of 22 basketball and handball players towards mouthguard wear
Out of the 45 players (all sports together) 44.4 % used a mouthguard, and 55.6 % used no mouthguard. The reasons for not wearing a mouthguard are shown in Figure 2.
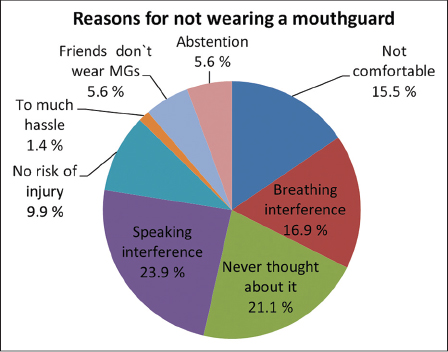
Figure 2: Distribution of reasons (n= 70) given by 45 players for not wearing a mouthguard
Distribution of Orofacial Injuries
62.5 % of the basketball players had previous orofacial injury, in 57 % soft tissue injuries (lip or cheek laceration), and in 43 % hard tissue injuries occurred (mandible luxation, tooth fractures, or tooth loss; each 14.3 %). After tooth fracture one basketball player (29 years old) got a professionally fitted mouthguard made by his dentist. His current mouthguard was 1.5 years old. He always wore it, in training sessions as well as in games. He was convinced about its protective role and injury prevention.
50 % of the handball players had no previous orofacial injury, whereas 18.7 % suffered from lip/cheek lacerations, concussion (12.5 %), tooth fracture (12.5 %), and jaw fracture (6.3 %).
In field hockey the wear of a mouthguard was compared for those who had or had no previous orofacial injury. 70.8 % (n= 17) had no previous orofacial injury, 4 players sustained lip/cheek laceration and 2 had a concussion. From 19 players who used a mouthguard 3 had lip/cheek laceration and no other dentofacial injury. Concussions and orofacial laceration occurred in 3 from 4 players who never had used a mouthguard.
28 (62 %) of all participants had no orofacial trauma experience. The remaining 17 players reported 22 injuries; multiple answers were possible. The most common injuries were lip/cheek lacerations (22 %). All answers are given in Figure 3.
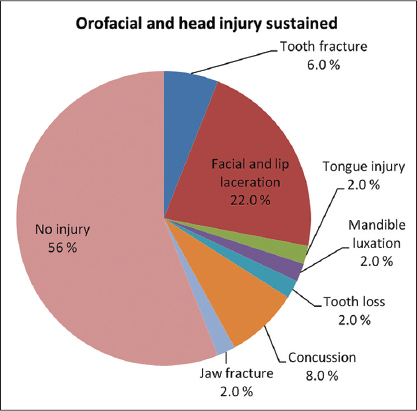
Figure 3: Distribution of no injury and trauma and orofacial injuries occurring in handball, basketball and field hockey together (Answers: n= 50)
The distribution of orofacial injuries is given separately for handball, basketball, and field hockey in Table 1. In field hockey, the injuries are related to mouthguard wear.
Table 1: Distribution of orofacial injuries
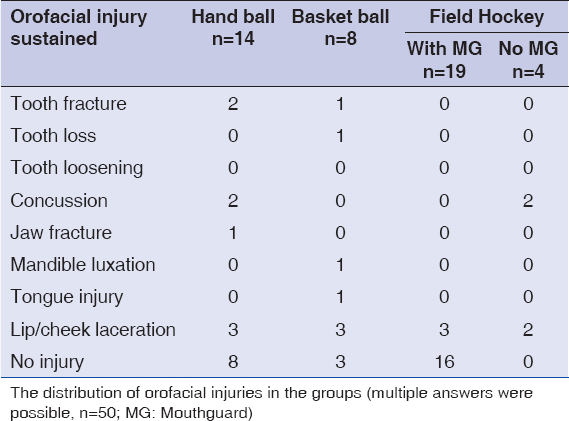
The distribution of orofacial injuries in the groups (multiple answers were possible, n= 50; MG= mouthguard)
RESULTS FOR THE ASSESSMENT OF THE PROVIDED AND TESTED MOUTHGUARDS IN BASKETBALL AND HANDBALL
In a scale from 0 (bad) to 10 (excellent) the vented Nike adult max intake mouthguard (VentMG) and the two-component mouthguard (MixMG) were evaluated in the handball and basketball players concerning the fitting, stability in running, comfort, interference in breathing, speaking, and drinking. The assessment was given after a sports specific physical agility test and after a game and analyzed together, because no significant differences were observed (Table 2). The interference of speaking was rated worse than all other parameters, and the impact on speaking ability was classified significantly worse for the VentMG (p< 0.005).
Table 2: Evaluation of mouthguard characteristics for BBHo (field hockey) versus VentMG and MixMG (basketball and handball) after a physical agility test and a game
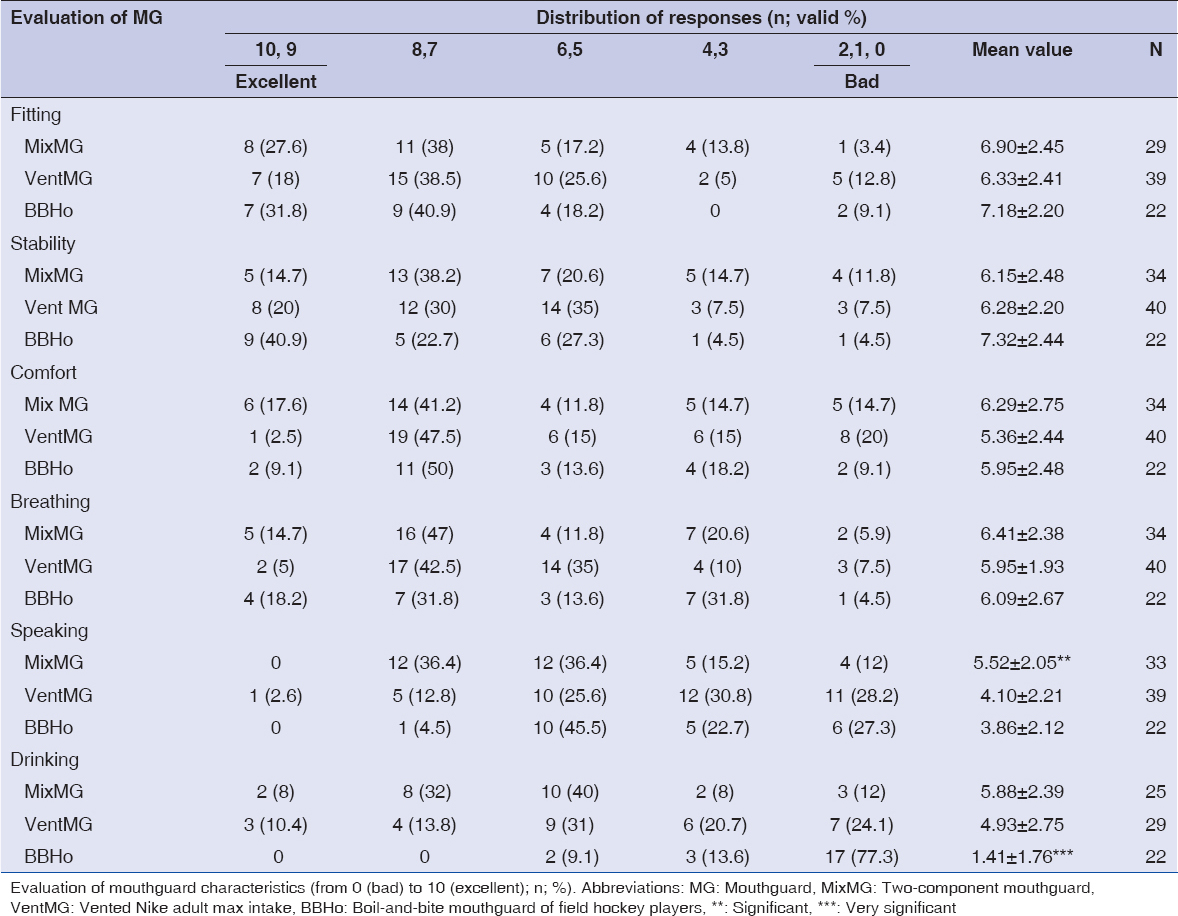
The perceptions of comfort, interferences, and stability of the two provided study mouthguards were compared to the usually worn mouthguards of the field hockey group. One female field hockey player was excluded from the assessment of mouthguard comfort because she had a professionally fitted mouthguard. The boil-and-bite mouthguard (provided by the club; Dita Multi Sport) of the remaining 22 field hockey players was compared to the reviews of the two study mouthguard types (Nike vented adult max intake (VentMG) and the two-component mouthguard (MixMG)) (Table 2). Perceptions of the ability to communicate and drink were consistently the most negative. The interference in speaking with the MixMG was characterized as significantly less, when compared to the boil-and-bite mouthguard of the field hockey players (p< 0.003), and VentMG (p< 0.005). The interference in drinking was markedly worse for the boil-and-bite field hockey mouthguard than for the two study mouthguards (p< 0.0001).
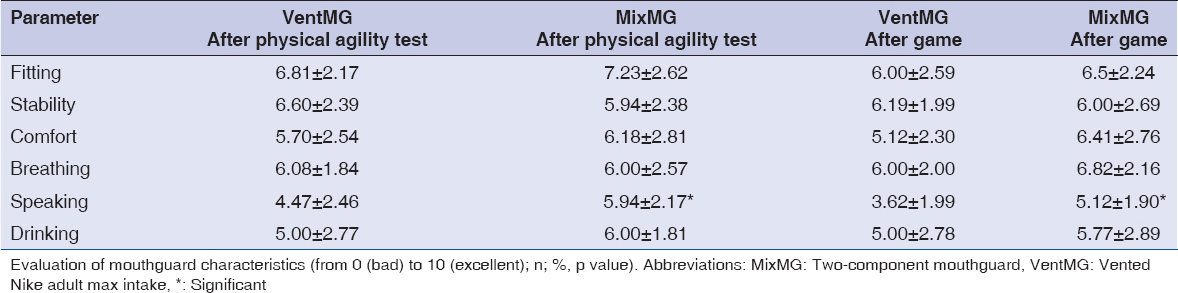
A comparison between the two study mouthguard types showed a significant difference in the interference in speaking which was higher in the VentMG wear (p<0.05 vs. p< 0.02) (Table 3). No significant differences were seen in the categories of fitting, stability on running, comfort, and breathing, classified in an average of 5 to 7 from 10 (Table 3).
Table 3: Evaluation of mouthguard characteristics for VentMG and MixMG separately after the physical agility test and game
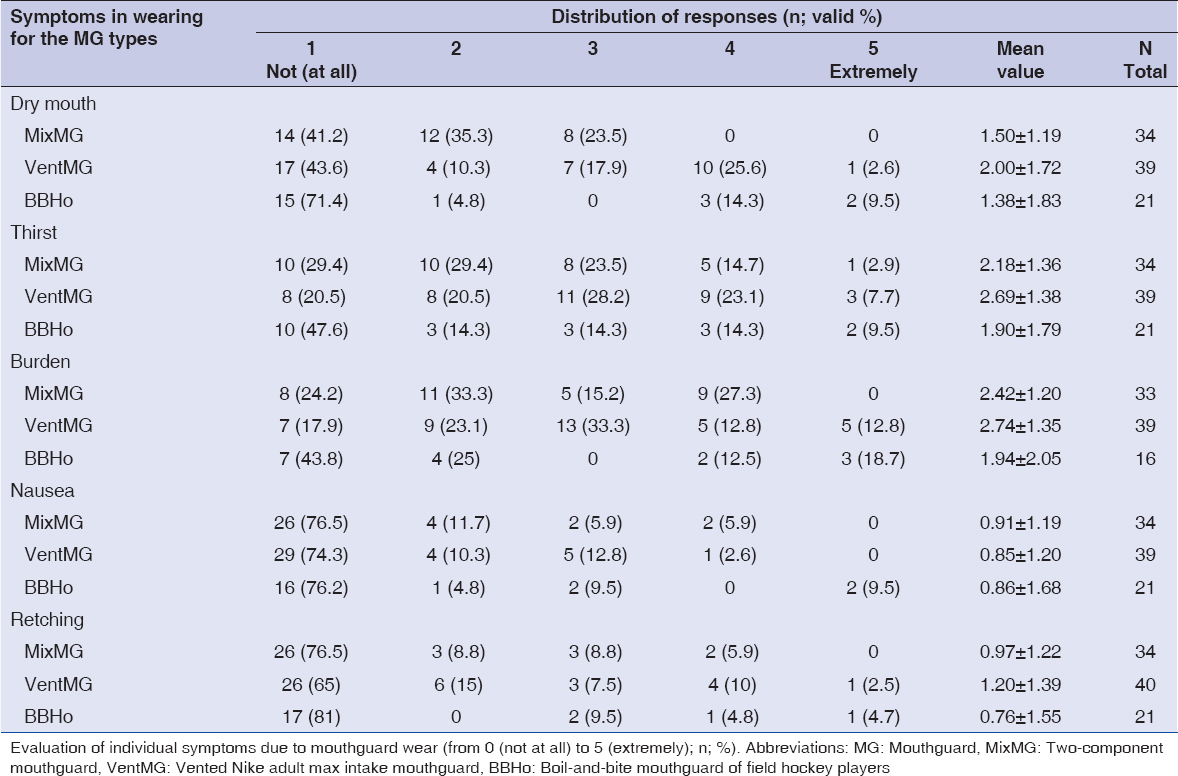
In a scale of 0 (not at all) to 5 (extremely) the players should rate the mouthguard for dry mouth, thirst, burden, nausea, and retching. No significant differences between the mouthguard types were oberserved (Table 4).
Table 4: Evaluation of BBHo (field hockey), versus VentMG and MixMG (basketball, handball) after the physical agility test and game concerning individual symptoms in wearing
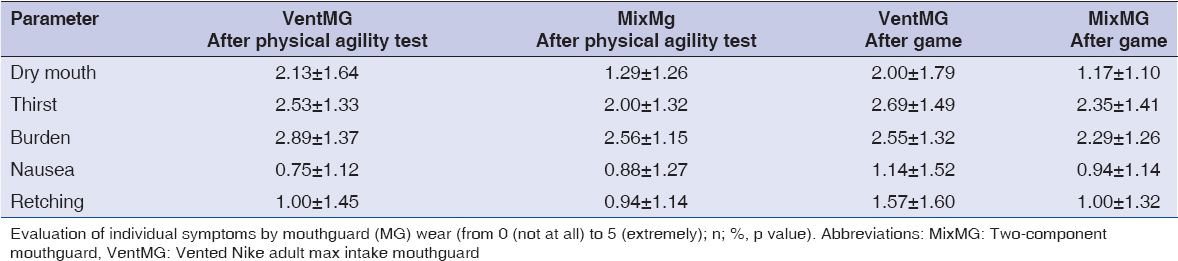
No significant differences concerning individual complaints were found between the VentMG and MixMG after physical agility tests and after games (Table 5). Also no significant differences were found in the categorization of characteristics for each mouthguard between physical agility test and game in unpaired as well paired (only in handball) testing.
Table 5: Evaluation of individual symptoms in VentMG and MixMG wear separately after the physical agility test and game
DISCUSSION
In this investigation the acceptance of mouthguards in basketball, handball, and field hockey as well as the frequency of orofacial injuries was checked. We compared the effects of a vented and two-component mouthguard on physical agility in handball and basketball players, who had no mouthguard experience, and the impact of these mouthguards in comparison to the regularly worn boil-and-bite mouthguard of field hockey players on game activity.
Mouthguard Acceptance, Reasons for Use or Rejection
The present study shows a marked cognitive dissonance between the attitudes of players and their reported behavior in mouthguard wear. While all basketball players and 71.4 % of the handball players acknowledged the value of mouthguard in injury prevention, only one basketball player used a mouthguard after previous tooth fracture, and no one from the handball group.
82.6 % (n= 19) of the field hockey players (78.3 %; n= 18) used a boil-and-bite mouthguard and 1 female field hockey player an individually fitted mouthguard for protective reasons (85.7 %), and 14.3 % because of other player's behavior. There was active encouragement and promotion by the hockey club to use boil-andbite mouthguards regularly. The selection of the mouthguards used and provided in the hockey club may be influenced by limited knowledge of the attributes and low cost of this mouthguard (~5.95 €). Because of the regular replacement, particularly in adolescents, the low cost may be relevant, and a professionally fitted mouthguard may be a too high financial barrier. The characteristics of different types of mouthguards may not be well understood by team members or coaches, who were the most frequent source of advice (66.6 %) after family and friends (29.2 %). The mouthguard use in field hockey was the result of the education and motivation of players, parents, coaches, and officials, supplementing the information to players. A most relevant role of coaches for mouthguard use has been described (17). In contrast Cornwell et al. (16) found that club and coach (18 %) played a less relevant role for mouthguard use vs. friends and family (49 %), especially in young athletes, followed by dentists (29 %).
In the basketball and handball teams, the active encouragement and promotion of mouthguard use by coaches or clubs was found to be very low, and this is in line with Berg (1998) and Collins (2015) (18, 19). The latter reported that coaches (87.3 %) or parents (64.5 %) had never recommended the use of a mouthguard.
In our present study almost all handball and basketball players wore no mouthguard. The most frequent reason was “never thought about this” (31 % in basketball, 27 % in handball), followed by “speaking and breathing interference” (23 % respectively 27 %). 7.6 % of basketball and a double percentage of handball players answered that they did not feel at high risk for dental injuries. The fact that the most frequent reason was “hadn't thought about it” is important for dentists, coaches, clubs and family members, and highlightens the lack of encouragement and promotion by the dental profession and player's organizations.
Collins et al. (19) examined the behavior, attitude, and current mouthguard use in basketball and softball athletes in 21 High Schools. The most frequent reasons for not wearing a mouthguard were “not necessary” (65.3 %), and “speaking and breathing interference” (61.5 %). Cornwell et al. (16) found that basketball players with previous injuries were 2.76 times more likely to use a mouthguard than those without previous injury. In our study only one basketball player always wore a mouthguard after sustained a tooth fracture, while the other basketball players had soft tissue injuries (n= 4) and a mandible luxation (n= 1) and used no mouthguard. In handball 12.5 % of the players had a tooth and 6.3 % a jaw fracture, but no behavioral change occurred and no one actually wore a mouthguard. The use of a mouthguard may prevent or attenuate dental and oral injuries. Despite their positive effects, mouthguards are rarely used. Obviously also former accidents had no relevant effect on the willingness to use mouthguards. This shows that new motivating tools must be developed to improve the acceptance for mouthguards in the future.
In basketball 50 % and in handball 14.3 % believed that mouthguards are necessary in games, and no one, except the only basketball player with an individual mouthguard, thought that mouthguards are necessary in training sessions. Collins et al. (19) found in a total of 1.636 basketball and softball athletes (12.3 %) who permanently or occasionally wore a mouthguard during training periods or competitions. The Australian intervention study of Cornwell (16) reported about the use of mouthguards in basketball. A total of 496 basketball players answered two questionnaires (baseline and follow-up). Players were youths (n= 208, 12-15-year olds) and adults (n= 288, 18 years and over) from all levels (social to elite). Completion of the baseline questionnaire was followed immediately by an intervention, comprising written and verbal informations about mouthguard wear and construction. Only 25 % (n= 125) used a mouthguard. The mouthguard wear was less frequent in training (25 %) than in the games (62 %). Despite the twelveweek intervention, the use of a mouthguard in young athletes did not increase, among adults by only 14 % for training and 10 % in the games.
In contrast we found in field hockey that 81.8 % of the players believed that mouthguards are necessary in games and (68.2 %) in training sessions. Accordingly 84.2 % always wore a boil-and-bite mouthguard in the games. In contrast only 50 % of the players who rated the mouthguard as necessary in the training wore a mouthguard in the training sessions. This demonstrates a marked cognitive dissonance between the attitudes of players and their reported behavior for the mouthguard use in training. In practice the training situation was assessed to have a lower importance and comfort restrictions were superior: As reasons for not always wearing a mouthguard were given speaking and breathing interferences (52.8 %), uncomfortable wear (16.7 %), “never thought about it” (14 %), no high risk for dental injury (8.3 %), and “friends also don't wear” (5.6 %).
The data on sports-related dentofacial injuries illustrate the need of mouthguard use in sports. It has been found that the incidence of injuries in handball is at approximately 13.5 per 1.000 hours athletic exposures (20). In contrast, the incidence of injuries in training was 0.6 to 2.6 per 1.000 hours. In basketball a range of 9 injuries per 1.000 competitions and in the training a range of 4 per 1.000 athletic exposures have been reported. Dental injuries occurred surprisingly often (21). According to an American study ((NCAA) at hockey players an injury rate of 6.3 per 1.000 athletic exposures accounted in training and competitions (22). These studies agreed that at higher leagues the number of injuries increased, as well as in training fewer injuries than in the competition occurred.
In a study by Collins et al. (19), the distribution of dental injuries was described in high school athletes between the years 2008 to 2014. Most dental injuries of the girls occurred in field hockey (3.9 % of all injuries) and of the boys in basketball (2.6 %). The injury rate in the training sessions was three times lower than in competitions. The most frequent causes of injuries were a blow from another player (61.3 %), and from the equipment (31.5 %). In 72.5 % of cases with a dental injury, the player wore no mouthguard. In case of mouthguard use in 96 % a “boil-and-bite” mouthguard was used, which is in line with our study concerning the field hockey players.
Frequency of Orofacial Injuries
From 23 field hockey players, 19 (82.6 %) were wearing a mouthguard at the time of the injury while 3 lip/ cheek lacerations and 2 concussions occurred, but no dentofacial injuries. Since a greater force is needed to produce dento-alveolar injuries in the presence of a mouthguard, it is speculated that some of these injuries were lessened or further injuries were prevented by the mouthguard. 4 field hockey players wore no mouthguard and 3 of them sustained concussion and orofacial lacerations. In total 70.8 % (n= 17) had no previous orofacial injuries.
In the handball group (n = 14) 50 % had orofacial injuries, 18.7 % sustained soft tissue lacerations, followed by 12.5 % with concussion, 12.5 % with tooth fracture and 6.3 % with jaw fracture (n = 18.8 % orofacial injuries). One study in Turkish elite handball athletes (23) found a slightly higher percentage (26 %) of the handball athletes who experienced at least one type of dental injury, and no one wore a mouthguard. Another study (24) at paediatric handball players (mean age 12 ± 1.6 years) in Turkey showed also in the rage of 19 % dental injuries, while no player used a mouthguard. The risk of injuries in handball is extremely high due to the dynamic and powerful stressed game character. Fast and strong-stretching movements with many changes of the direction and frequent opponent contacts make the game attractive and exciting for the spectators. Due to direct and partly hard contacts with the opponents a relevant risk of traumatic injuries is always present. In particular aggressive behavior with pushing and pulling while attacking an opponent may cause many injury cases. Throws at the goal which are influenced by external conditions can miss their target from time to time and cause serious injuries to the head and face.
In the basketball group of our study 62.5 % (n= 5) had orofacial injuries, suffered soft tissue lacerations (n= 4), and dentaloral injuries (n= 3).
Basketball is a high impact sport with high prevalence of orofacial trauma, particularly maxillary central incisor and lip injuries, but athletes did not use mouthguards.
Orofacial injuries in basketball are frequent. Approximately 10 % of all injuries in basketball involve the head, neck, or orofacial area (25). A prospective study at Minnesota high school basketball athletes reported a high proportion of orofacial injuries (55.4 % of the players per playing year), and a study at 1020 high school varsity basketball players in the US recorded 30.9 % injured players (26, 27). The distribution of injuries included: Lacerations, 49.9 %; facial bruising, 15.8 %; loosening of teeth, 10.9 %; jaw stiffness, 10.3 %; numbness, 5.7 %; and fracture; 0.2 % (26). Excluding Rugby Union, a New Zealand study found basketball to be the third highest contributor to dental injuries compared with the top 10 sports (28). A study of 246 schoolboys in Singapore ranked basketball with the third highest prevalence of dental injury (29).
A study of the Brazilian National Basketball players (30) showed in 50 % orofacial injuries, dental trauma accounted for 69.7 %, with emphasis on maxillary central incisors, followed by soft tissue (60.8 %, mostly lip injuries). Only 1 % wore a mouthguard at the time of trauma.
Knobloch et al. (31) studied in school sports (School Year 1996/97, Germany) the distribution of injuries in different sports as well as the location of the injury. There were 2.234 violations registered of which 73 were related to the mouth and jaw area, which accounted for 3.3% of total injuries (in total, there were found in basketball 431 injuries, in handball 110, and in hockey 65). From these 73 orofacial injuries 51 affected the teeth (2.3 %). Related to the sports from these were found 7 tooth injuries in basketball, 1 in handball and 6 in hockey. In hockey, the dental injury rate of 9.2 % from the total was the third largest after bruises (n= 31; 47 %) and lacerations (n= 7; 10 %). In hockey 30.8 % of all injuries occurred in the head region, and mostly caused by a blow from the ball or stick (61.5 %).
In our study 58 % of all participants without mouthguard use had orofacial injuries, mostly soft tissue lacerations (59.6 %), followed by concussion (27 %), tooth fracture and loss (26.6 %), jaw fracture (6.6 %), and mandible luxation (6.6 %).
In contrast to many other body tissues, most dental tissues have a low potential for recovery, when damaged. A dental crown fracture is irreversible. Even a minor injury like a concussion can cause pulp necrosis. More severe injuries such as dislocations or avulsions may result in the loss of the tooth due to ankylosis or infection-related root-resorption (32). An injured tooth often requires extensive treatment just to become functional again and can create a lifetime of expensive, long-term problems for the athlete (33-35). For these reasons, the wear of a mouthguard is recommended. In terms of the high rate of orofacial injuries shown in this study the use of a mouthguard is necessary and can have a relevant preventive value.
Comfort
Player perception of the mouthguard is important as this largely determines the compliance and enthusiasm (6). The mouthguard should be comfortable, retentive, allow normal breathing and speech, and should not impinge on the soft tissues (36). Stock mouthguards are inexpensive, and are ready for immediate use. They are often ill-fitting and many strongly interfere with breathing and speech because they must be held in position by keeping the teeth together.
Mouth formed mouthguards are a compromise between stock and custom made, and inexpensive. The most popular is the boil-and-bite mouthguard type. Often it is made of a thermoplastic material, usually EVA copolymer. It is softened by boiling water and adapted intraorally while warm by biting into the material. Another version comes with a shell, usually of ethylene vinyl chloride. Mouth-formed mouthguards fit better than stock mouthguards.
Custom made mouthguards are fabricated indirectly on a stone model from a dental impression, usually alginate. These mouthguards are the most expensive but are superior in many aspects. A custom-made mouthguard has the superior comfort, breathing, fit, speech, protection, and performance. The costs after sports-related alveolar and dental injuries in mixed dentition are much higher than the repeated manufacture of individual mouthguards e.g., due to growing jawbones in children. To make mouthguards more attractive, they can be offered in different colours.
Problems associated with breathing, speaking, and comfort are unlikely to influence mouthguard selection unless the player has used one previously. Only one player in our study basketball group used an individually fitted mouthguard. The handball players used no mouthguard before.
Subjects using mouthguards consistently indicated that their breathing and speaking is impaired and they are uncomfortable (37). Other studies have cited discomfort and poor fit as common concerns (38, 39).
The results of this study support this conclusion, and mostly no perceptual significant differences were reported between the vented and two-component mouthguard evaluated from the handball and basketball players concerning comfort and subjective impressions. The interference of speaking was rated worse, and the impact on speech was classified significantly worse for the vented mouthguard (p< 0.005). This may be due to the breathing channels which may impair the lips and tongue. No differences were seen between the agility testing and game condition. The handball and basketball players with one exception in each group had no previous experience in wearing a mouthguard during sport activity; however, it is possible that regular or everyday use of a mouthguard could influence these perceptions.
The field hockey players wore their cheap boil-and-bite mouthguard mostly regularly during sport activity, and had much experience in this mouthguard model. We also compared the ratings of the experienced field hockey players to those of the basketball and handball players. The interference in speech with the two-component mouthguard was characterized as significantly less, when compared to the boil-and-bite mouthguard of the field hockey group (p< 0.003) and the vented mouthguard (p< 0.005). The twocomponent mouthguard may have a minor impact on speech because the soft mass adapted perfectly to the contour of each tooth, hardened in the mouth and got individualized. No significant differences were seen in the categories of fitting, stability on running, comfort, and breathing, classified in an average of 5 to 7 from 10. Interference with speech and drinking was rated the worst. The field hockey players regularly used a mouthguard during sport activity, but the regular use of the mouthguard resulted in no difference in the perceptions nor had a great influence when compared to the handball and basketball players who were unexperienced in mouthguard wear. The field hockey players rated the drinking ability of their mouthguard worse than the handball and basketball players. The individual symptoms in wearing (thirst, dryness, burden, nausea, and retching) rated in a scale from 0 (not at all) to 5 (extremely) resulted in categorizations between 1.5 to 2.5, and showed no significant differences between the sports groups.
Mouthguards can cause discomfort when placed in the oral cavity, in particular due to their thickness of the labial and palatal region to reduce the impact force of an injury. The mouthguard must dampen vibrations and be rigid enough to distribute the power. A good mouthguard combines the positive characteristics such as high protection, secure grip, long life, easy handling and purification, and above all it has not to affect the performance, breathing and speaking of the athlete. In Germany a study by “Stiftung Warentest” about different mouthguard types showed that the commercially available simple mouthguard, although it was the most cost effective solution (with 5 to 10 €), was classified as “unsuitable” (in the categories of fitting, mouth breathing, speaking, protection and acceptance). The variant “boil-and-bite” (between 5 and 40 €) was in all points of investigation classified as “less suitable”. The price of the two-component mouthguard (25 to 40 €) was similar to the boil-andbite mouthguard, but “suitable” in 4 of 5 estimated study points, only the point “protection” was classified as “less suitable” as for the boil-and-bite mouthguard. Only the custom-made mouthguard, from dentists or orthodontists prepared, and with 100 to 200 € a more expensive version, was rated in the test as “very useful” (fit, support, and acceptance) or classified “suitable”.
In our present study, we tested a boil-and-bite and the two-component mouthguard as a possible alternative to an expensive individual mouthguard and found only the speaking ability as significantly better in the twocomponent mouthguard.
The subjects' perceptions of the mouthguard is important as this largely determines their attitudes and behaviors. The individual ratings of the field hockey players who wore a cheap boil-and-bite mouthguard, did not significantly differ from those of the handball and basketball players. The mentioned discomfort and interferences could not affect their acceptance of their boil-and-bite mouthguard and its regular wear in field hockey games. This may be influenced by the coach and family members, who forced the mouthguard use as an ultimate influence. Despite all possible and obvious disadvantages, the use of a cheap boil-and-bite mouthguard was in the most field hockey players a tightly integrated behavior in their sports activity. Two female players reported that the wearing is a purely mental issue, because they feel uncomfortable in the game without their mouthguard.
This in summary demonstates, that education, information, strict instructions, and the assistance of club, coach, family and friends can obviously integrate a desired behavior (mouthguard wear) into daily sports, despite possible restrictions.
CONCLUSIONS
The acceptance and use of mouthguards must be markedly intensified in handball and basketball. Although all basketball players and 71.4 % of the handball players acknowledged the protective value of mouthguards, the most frequent reason for not wearing a mouthguard was “never thought about this”. In field hockey the use of mouthguards was common. 82.6 % acknowledged the protective value of the mouthguard. Its consequent use during the field hockey games was highly influenced by the education and motivation of players through parents and coaches. Health professionals themselves, including dentists, should be well informed about the sport specific value of mouthguards. This is crucial to increase mouthguard use in ball sports. Educational programs, media promotion and vertical dissemination of information within basketball and handball organizations could also be effective. Further investigations of dental injuries in hand- and basketball would be valuable in order to provide players, coaches, parents and sporting federations with the necessary information to make decisions regarding the use of mouthguards. Mouthguard use should be made compulsory, especially in these sports with high risk for dental injuries.